Advance Beneficiary Notice of Noncoverage (ABN) Form Instructions Tool
Hover over each form field to better understand this form.
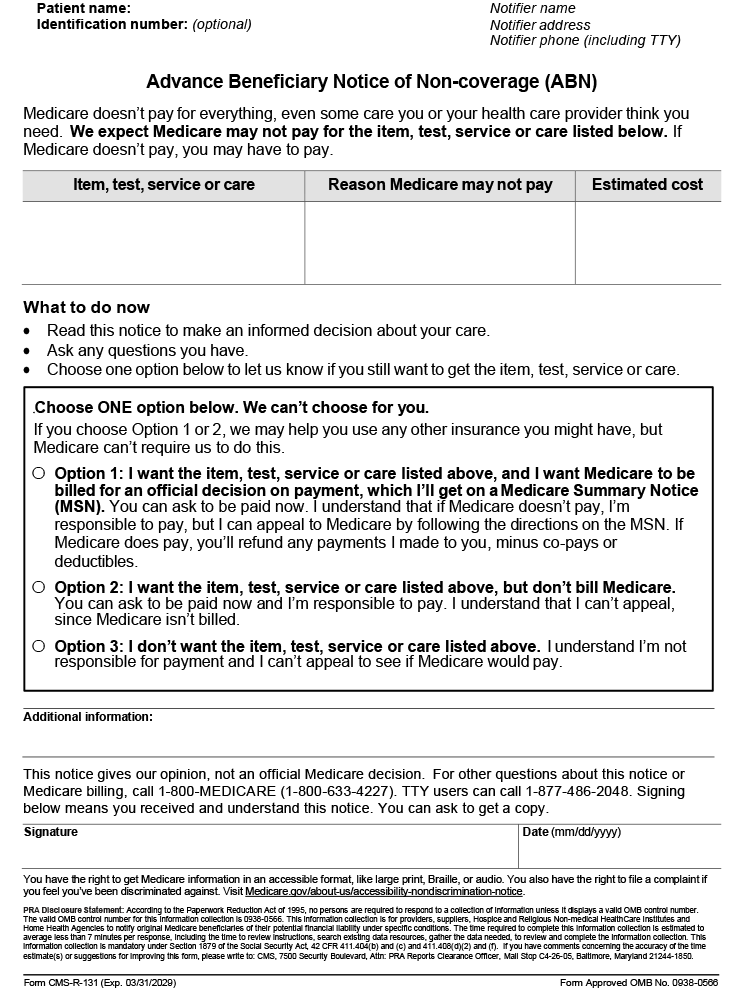
See FFS ABN | CMS![]() for additional information.
for additional information.

Advance Beneficiary Notice of Noncoverage (ABN) Form Instructions ToolHover over each form field to better understand this form.
See FFS ABN | CMS Disclaimer: CGS' online tools and calculators are informational and educational tools only, designed to assist suppliers and providers in submitting claims correctly. CGS makes no guarantee that this resource will result in Medicare reimbursement for services provided. Although we've made every reasonable effort to provide effective resources, CGS is not responsible for the consequences of any decisions or actions taken in reliance upon or as a result of the information that these tools provide. CGS is not responsible for any human or mechanical errors or omissions. |
| 26 Century Blvd, Suite NT600, Nashville, TN 37214 | © CGS Administrators, LLC. All Rights Reserved |
