


Prior Authorization for Repetitive, Scheduled, Non-Emergent Ambulance Transports (RSNAT)
This option allows you to submit a prior authorization request for RSNAT. See the Prior Authorization for RSNAT webpage for details about the prior authorization process.
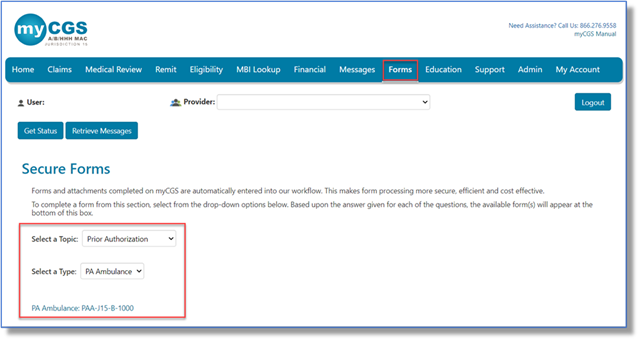
- Log in with a user ID registered to a Part B NPI/PTAN.
- Select the 'Forms' tab.
- Choose 'Prior Authorization' from the 'Select a Topic' drop-down selection.
- The 'Select a Type' drop-down selection will default to 'PA Ambulance'.
- Select 'PA Ambulance: PAA-J15-B-1000' at the bottom of the page.
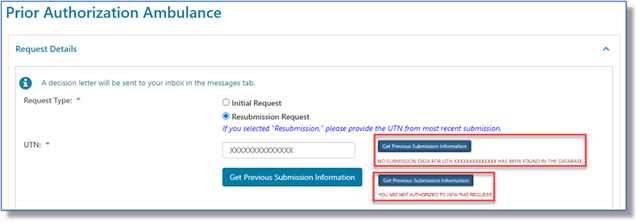
Request Details
Select the appropriate request type:
- Initial Request: First prior authorization request (PAR) submission.
- Resubmission Request: Any subsequent PAR submission (i.e., to correct an error or omission identified after receiving a non-affirmation decision).
- Enter the 14-digit Unique Tracking Number (UTN) assigned to the most recent PAR. (Select 'Get Previous Submission Information' to verify).
- Enter the 14-digit Unique Tracking Number (UTN) assigned to the most recent PAR. (Select 'Get Previous Submission Information' to verify).
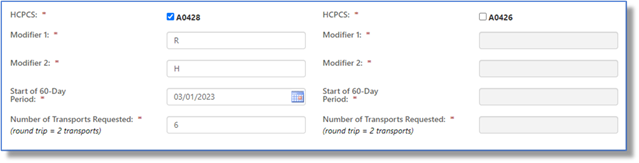
Select the appropriate HCPCS code(s) (A0428 or A0426) and enter the applicable origin/destination modifiers, start date, and number of transports.
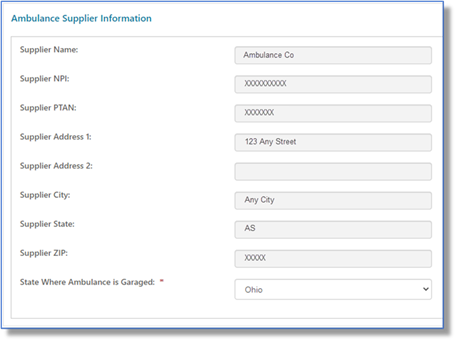
Ambulance Supplier Information
This section auto-populates based on your user ID. Exception: Select the state where your vehicle is garaged.
Beneficiary Information
Enter the beneficiary's Medicare Beneficiary Identifier (MBI), name, and date of birth.
NOTE: See the 'Eligibility' tab to verify and ensure the information you enter matches.
Certifying Physician Information
Enter the certifying physician/non-physician practitioner's name, identifiers (NPI/PTAN), and complete address.

Requestor Information
This section auto-populates based on your user ID. To receive the PAR decision via fax, check 'Send decision by fax' and enter the fax number.
Questions
Answer each service-related question to help support medical necessity and enter comments as appropriate.
Attachments
Select the 'Choose File' button to attach ALL supporting documentation. Attachments must be in PDF format and no larger than 40 MB each. The total for all attachments can't exceed 150 MB.
If you're ready to send the request, click 'Submit'.
The eSignature box will display. Before you select 'OK' (to sign and acknowledge that you're authorized to submit the information), verify that the displayed information and attachment(s) are correct.
If you need additional time, click 'Save'.
A confirmation message will display.
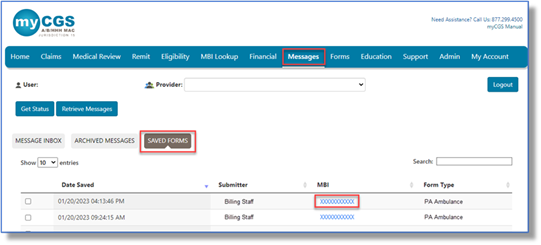
To access a saved form, go to your 'Messages' tab and select 'Saved Forms'. Select the form you want to load and update.
 Join Electronic Mailing List
Join Electronic Mailing List Print
Print Bookmark
Bookmark Email
Email Facebook
Facebook YouTube
YouTube LinkedIn
LinkedIn